
The New Zealand Vaccination Records Leak: A New Analysis by William Briggs and Some Lesser Thoughts of My Own

As everybody in this corner of the internet knows, a New Zealand Te Whatu Ora employee named Barry Young leaked four million vaccination records from New Zealand’s “pay per dose” vaccine programme to Steve Kirsch on 8 November. The records apparently pertain to doses administered to individual patients at apothecaries and doctors’ practices; vaccines administered by special mobile vaccination teams and at government mass vaccination centres were recorded separately and remain hidden from us.
Kirsch removed patient names from the data before providing a summary version to Norman Fenton and the full records to my friend William Briggs for independent review. Finally, on 30 November, he released the anonymised dataset to the internet and posted his own analysis to Substack, where he argues vigorously that the records show a vaccine-associated mortality rate of one death per 1,000 doses. This mortality rate would mean well over 13 million vaccine-induced deaths worldwide.
A lively Twitter debate has emerged about the significance of the data and their proper interpretation. Further drama has visited the real world. Young, the leaker, was arrested on Sunday for “dishonestly accessing Te Whatu Ora databases.” He faces up to seven years in prison, and was released on bail yesterday. Meanwhile, the New Zealand Ministry of Health secured a court injunction to stop the distribution of the leaked data, and used this authority to close Kirsch’s Wasabi file server. Friend-of-the-blog Kevin McKernan, who had agreed to mirror the dataset, likewise had his account with the file hosting service MEGA deleted with no notice, and at considerable personal and professional cost. These measures are of course contemptible and they will do nothing to stop the further spread of the leak, which is now all over the internet.
Some of you have asked me for my thoughts about the leak, but I didn’t want to say anything until Briggs posted his analysis, because his work has always been very important to me. I am pleased to say that he has now published his full, in-depth report. I encourage you to read the whole thing, and also to subscribe to his Substack. You won’t regret it:

See also his Twitter thread, where he summarises the most important points.
As for my thoughts:
1) New Zealand has reacted harshly against the leaker and against those who have hosted the leak, even in its anonymised form. This reaction cannot, in itself, be used to argue that there must be evidence of mass vaccine mortality in this dataset. I don’t know anything about New Zealand law, but I would not be surprised to find that the unauthorised release of non-anonymised patient records is a crime there. This not a comment on the justice of Young’s arrest, merely an observation. It is highly likely that New Zealand health authorities themselves are uncertain about what lurks in their vaccine records and what random internet people might find in them. Clearly they have been stupid enough to trigger the Streisand Effect by deleting the accounts of Kirsch and McKernan, so we should not expect too much of them. It is also possible that there are things other than vaccine mortality lurking in these numbers that they want to keep hidden from the public and that the internet has yet to discover. Finally, bureaucracies fight ferocious battles to keep even the most mundane records secret, because the mere pretence of access to hidden information allows state officials to make statements that outsiders cannot challenge or verify.
2) I was fairly certain from the beginning that there would be nothing all that dramatic in these records, because the possibilities are bounded firmly by all-cause New Zealand mortality statistics.
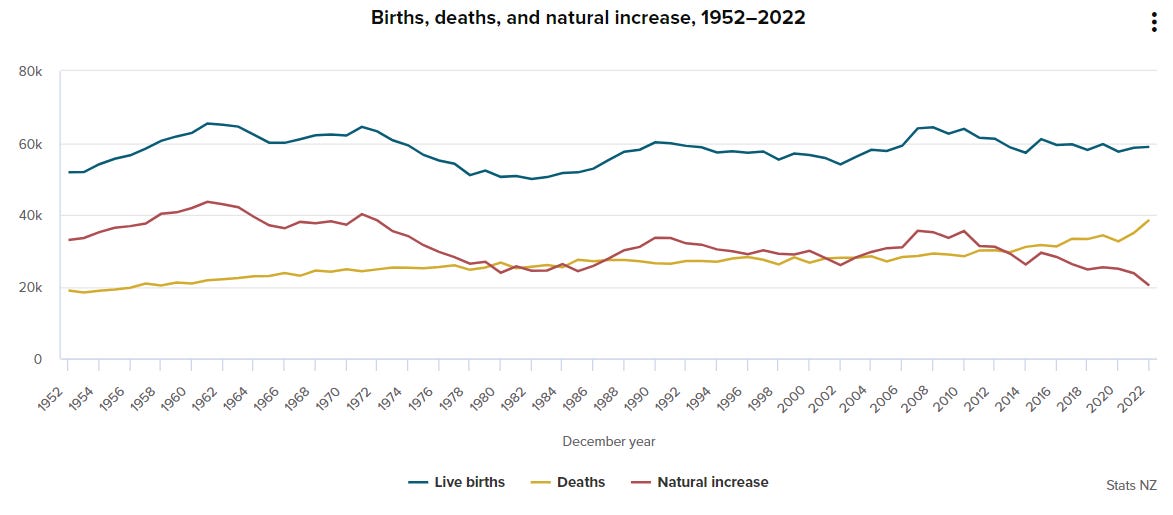
Consider all-cause mortality in New Zealand for the past five years:
2023 is not over yet, but 37,569 deaths have been counted there through the twelve-month period ending in September of this year. This is somewhat lower than the 38,052 deaths recorded year-to-date in September 2022.
New Zealand effectively shut itself off from the world in 2020 in an effort to stop Covid, and their measures inevitably stopped a lot of other viruses too. At great cost, they seem to have saved about 2,000 lives in the short term, accounting for the anomalously low death numbers in 2020. The elevated death numbers for 2022 – the year the pandemic reached New Zealand – are officially the fault of Covid, but some of them must simply represent a compensatory rise from the low point of 2020, because viruses tend to kill the very old and the very sick, and these people have to die sometime. In 2022 and 2023, I can see room for an absolute maximum of 8,000 excess deaths. Probably 2,000 of these are sick and frail people who would’ve died in 2020 had it been a normal year, and so we’re left with at most 6,000 deaths to divide between the arrival of Covid, the return of other viruses and the vaccines. This is remarkably close to the official Covid New Zealand death count, which is currently at 5,143.
It’s simple, then: How much room you think there is for direct vaccine mortality will depend on how much you dispute these official Covid death numbers. I propose that any more than 2,000 vaccine deaths is just not very plausible. Certainly, there is no way to make Kirsch’s estimated vaccine mortality rate of one death per 1,000 vaccinations work with these numbers. New Zealand has administered 12 million doses, which would mean 12,000 vaccine-induced deaths. I see no room for that kind of mortality here.
Some will surely object that the mortality numbers cannot be trusted, but if that’s the case, we are totally in the dark and we don’t know anything. Even if you want to argue that all Covid deaths are reassigned vaccine deaths, we still don’t have the numbers to make the math work. Of course, all of this applies only to direct vaccine mortality; some of the Covid deaths could be down to immune imprinting from the jabs or other transmission-enhancing effects, but these are somewhat different questions which the leaked data won’t help us answer.
Briggs makes many important points, and I again encourage you to read his entire piece. Here I only want to highlight the most crucial part of his analysis, where he explains how the leaked records contain “misleading signals” that at first glance suggest high vaccine mortality, but that are actually mostly an artefact of sampling.
He provides this histogram, of the number of deaths after just one jab, after just two jabs, after just three jabs, and so on. In every case, there appears to be a mortality blip immediately following vaccination. This looks at first like the vaccines are killing a lot of people.

In fact, it is largely an illusion caused by the nature of the data, which do not continue to the present or into the future, but stop in early October 2023. Basically, we cannot see mortality more than 850 days out from the earliest jabs, and this causes deaths to artificially cluster in the early days post-jab.
This is a little hard to explain, so bear with me: Pretend we’re studying the immediate mortality caused by a benign vitamin pill (which should not kill anyone), and our dataset covers only ten days. People can take the pill at any time – on day 1, on day 2, on day 7, or on day 10. Some random number of them may die of totally unrelated causes on any day after taking the pill. People who take the pill on day 1 have ten days to die. Their deaths can occur on any day post-pill – one day post-pill all the way up to nine days post-pill. People who take the pill on day 9, however can only die one day post-pill. Otherwise their deaths will be invisible to us. Because of these stragglers, you’ll end up counting more deaths in the early days after taking the pill, because your dataset is more complete for the early days post-pill than it is for the later days post-pill.
All of that said, Briggs also notes that this sampling artefact is not the only thing going on in the data. There does appear to be some unusual clustering of deaths in the early days after the first and second jabs, particularly in people under thirty years of age. We’re talking hundreds and not thousands of deaths here, but I think it’s very plausible that this is a real signal of direct vaccine-induced death, precisely in those age cohorts at least risk of Covid mortality. This is similar to mortality effects suggested by an exhaustive study of German mortality data I posted about last year, and if this can be confirmed, it would be a great scandal, because the vaccines do not stop transmission and there was no reason to risk the lives of young people with our deranged mass vaccination campaigns.
UPDATE: I suspect there’s another selection effect at work in the clustering of post-jab deaths in the immediate aftermath of jabbing. Here’s Briggs’s histogram again, of days post-jab on the x-axis, and number of deaths on the y-axis. I’ve circled in green all those deaths that occurred about a month out from vaccination.
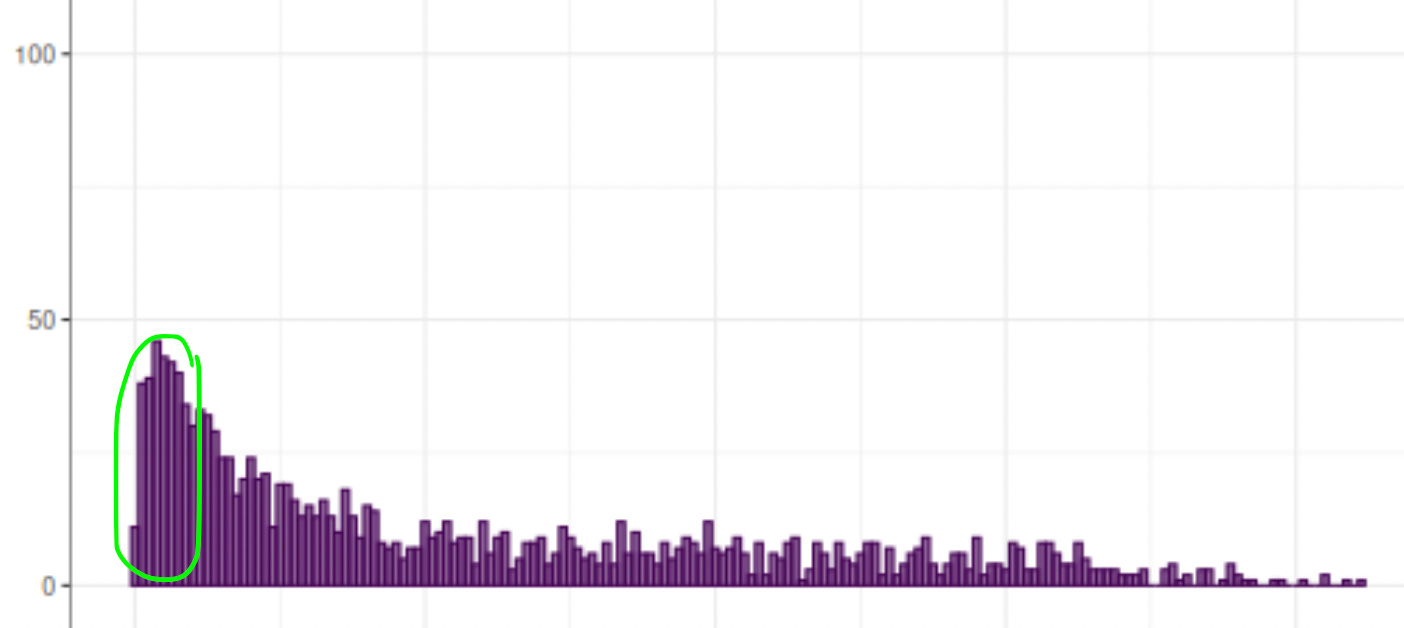
These are people who only got one jab. This is rather unusual, and I suspect many of them were jabbed only once because they did not survive to their second jab appointment. Perhaps the vaccines killed some of them, but we’d see some drop-off in deaths after a few weeks even if the jabs were as harmless as vitamin pills, for the simple reason that those who lingered a week or two longer to get jabbed a second time are counted as two-jab deaths instead and are not in this chart.
UPDATE 2: Some dispute my observations about all-cause New Zealand mortality. Kirsch argues that there have been 10,000 excess deaths from 2021 to 2023. He gets this number by subtracting mortality totals for these years from the total mortality New Zealand saw between 2017 and 2019. OECD, which uses the past five-year mortality average to calculate excess deaths for every year, arrives at even higher excess death numbers for the period of the pandemic.
The problem is that these aren’t defensible ways to calculate excess mortality for New Zealand. Two things above all drive all-cause death figures: 1) overall population size, and 2) the size of older demographics. New Zealand is a small country with both an increasing overall population and an increasing population of old people. This means that using pre-pandemic years as a baseline will overstate substantially the number of excess deaths.
In 2019, 34,260 people died in New Zealand – an increase of 1,305 deaths compared to 2018. If we look at the specific death rates for those aged 65 and older – who account for 80% of all deaths – we see no unusual trends:
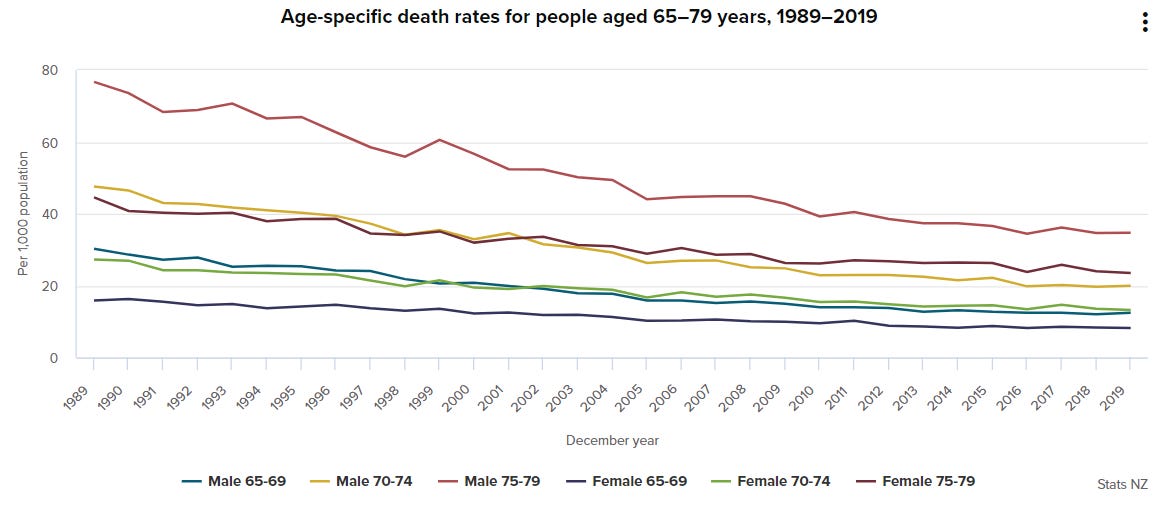

2019 was therefore a normal year, and because New Zealand only got more populous and older from 2020 to 2023, we would expect all-cause mortality even without Covid or vaccines to increase somewhat for each of these years. I’ve tried to be as generous as possible in my estimation that we’re looking at about 6,000 excess deaths over the entire period of the pandemic, but even if you think Kirsch is right in estimating 10,000 excess deaths between 2021 and 2023, that is not enough to support a vaccine mortality rate of one death for every 1,000 jabs. He is still 2,000 deaths short, and some of his excess will be Covid deaths and additional compensatory mortality for the low mortality of 2020.
After reading this full post but not reading the underlying analysis yet (I do have a day job), I have to say that I generally agree with the conservative position that our host is taking. Given the enormous numbers of vaccines given out, a death rate of 1 in 1000 would be immediately apparent, I would think.
But I do have two caveats to that, or areas for additional investigation, or however you want to call it.
First: mortality isn't the only thing we care about. There are fates other than death, after all. The shots might have disabled people or generally cratered their quality of life, without killing them.
I know I'm preaching to the choir but over the past year, a _lot_ of people I know who were generally pro-vaccine and denied any risks, have told me that they have suffered fairly severe health issues in the past few years. Maybe 2/3rds of these people straight up say they believe it was the vaccine. The remaining 1/3rd don't believe it was the vaccine, but I do.
Most of them are citing heart-related issues, which makes perfect sense given what we've known about the spike protein since April of 2020. But some of them have been fairly severe. One guy I know was hospitalized for a month. Another guy has been dealing with moderate health problems, enough to make him routinely miss social events, for over a year now. Five or six others I know have ambiguously referred to issues without sharing details. And these are just the people who have told me this in person. The numbers jump the dozens if I include internet friends
Second: The vaccine disability stuff has made me really appreciate just how well the authorities can suppress inconvenient information if they want to. I legitimately thought that everyone around me was still getting boosters every six months, until last April. I was laid off from my job, and somewhat pissed about it, and went filter-off in work chat. One of the first things I said was something like "FUCK ALL OF YOU FOR THE LAST FOUR YEARS OF DISCRIMINATION AGAINST ME. I NEVER TOOK A VAX". Three of the eight people on my team at work DM'd me to say "I wish I had not taken it, I've had health problems ever since", and this made me realize that there's been a preference cascade and it just happened quietly.
That, plus finding out in the past six months how many of my friends are suffering moderate to serious disabling health problems, has made me think. After all, they've all been suffering these since 2021. Somehow even me, with my paranoid conspiracy theorist brain, missed this. The government successfully suppressed this information from me, and even talking to close personal friends who had had this experience first hand, it took me two years to find out.
So, honestly, maybe 20 million americans have died of covid vaccine, and all the numbers are lies, and the authorities have somehow successfully hidden this. It sounds insane, but this _literally happened_ with covid vaccine _disabilities and nonfatal health issues_. So at this point my epistemic foundation is so thoroughly fucked that I could believe just about anything
Your analysis appears sound. I would say that even one or two thousand deaths in New Zealand because of the jabs would be a terrible result and should be more than enough to revoke any authorization immediately. Solidly proving such a conservative number would, in my opinion, be much more useful than falling prey to any exaggerations. „Wer zuviel beweisen will, beweist nichts!"